Pregnancy Support Medications: Ensuring Uterine Preparedness After Embryo Transfer During the Luteal Phase
In assisted reproductive technologies (ART), maintaining the uterine lining and adequate progesterone levels after embryo transfer is crucial for successful implantation and pregnancy. Luteal phase support (LPS) involves the administration of medications to sustain the endometrial environment post-transfer.
Below is an overview of commonly used medications, including their mechanisms, usage, and considerations.
Progesterone Preparations
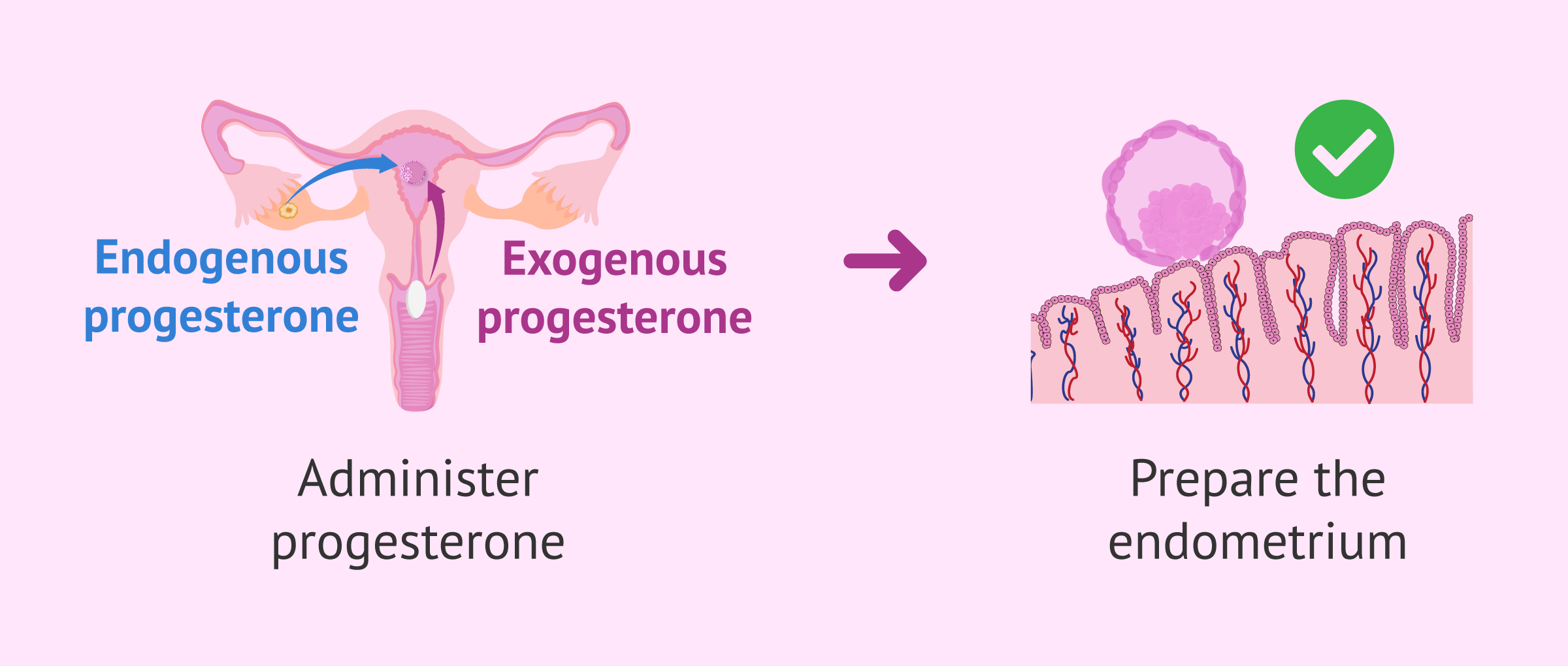
Progesterone is essential for preparing the endometrium for embryo implantation and maintaining early pregnancy. It can signal for embryo implantation and decidualization (the process by which endometrial stromal cells transform into specialized decidual cells in preparation for and during). Various formulations are available, each with unique characteristics.
Endometrin (Progesterone Vaginal Inserts)
Mechanism: Provides exogenous progesterone directly to the vaginal mucosa, ensuring localized delivery to the uterus.
Usage: Inserted vaginally, typically twice daily, starting after embryo transfer.
Considerations: Effective in maintaining the luteal phase; however, some patients may experience vaginal discharge.
Crinone (Progesterone Gel)
Mechanism: A vaginal gel formulation delivering progesterone directly to the uterine lining.
Usage: Applied vaginally once daily, beginning after embryo transfer.
Considerations: Offers convenience with once-daily dosing; may cause vaginal irritation in some users.
Prometrium (Oral Progesterone)
Mechanism: Micronized progesterone administered orally to support the luteal phase.
Usage: Taken orally, usually twice daily, starting after embryo transfer.
Considerations: Less commonly preferred due to variable absorption rates; may be used when vaginal formulations are not suitable.
Progesterone in Oil (PIO)
Mechanism: Intramuscular injection of progesterone dissolved in oil, providing sustained release.
Usage: Administered intramuscularly, typically daily, after embryo transfer.
Considerations: Effective in maintaining progesterone levels; associated with injection site discomfort and requires proper technique.
Look below for an example image of what progesterone medication can help with!
Reference - https://www.invitra.com
Estradiol (Estrace)
Mechanism: Synthetic form of estrogen used to support the development and maintenance of the endometrial lining.
Usage: Administered orally or vaginally, starting prior to embryo transfer and continued post-transfer.
Considerations: Supplementation may be necessary in cases of insufficient endogenous estrogen production.
Additional Medications
Dydrogesterone
Mechanism: A synthetic oral progestin that supports the luteal phase.
Usage: Administered orally, often in combination with vaginal progesterone.
Considerations: May offer an alternative for patients intolerant to vaginal progesterone.
GnRH Agonists (e.g., Leuprolide Acetate)
Mechanism: Initially stimulate and then suppress gonadotropin release, aiding in luteal phase support.
Usage: Administered as a subcutaneous injection during ART cycles.
Considerations: Usage is debated; some studies suggest efficacy, while others report limited benefit.
Conclusion
Luteal phase medications, primarily progesterone, are essential for maintaining the secretory phase of the endometrium, which is critical for embryo implantation and early pregnancy support. Progesterone promotes the transformation of the endometrial lining, making it receptive to the implanted embryo, and inhibits uterine contractions that could otherwise expel the embryo. Without adequate luteal phase support, the insufficient production of progesterone can lead to inadequate endometrial development and an increased risk of early pregnancy loss or failed implantation.
“Didn’t need this stuff back in my day!”